Total Hip Replacement is an extremely successful surgical procedure to improve a patient’s quality of life when arthritic hip pain becomes debilitating.
Hip replacement surgery offers patients the ability to return to their daily (and some sporting) activities without pain and with improvement in hip flexibility and movement. Patients with a significant limp as a result of an arthritic hip will often walk normally again after recovering from surgery.
The timing of surgery is a quality-of-life decision and it is never too late to replace the hip joint provided one’s general health is satisfactory.
There are various approaches that surgeons use to replace the arthritic hip.
All recognised surgical approaches work. Using tried and tested Hip Replacement designs, there is more evidence now that suggests a hip replacement may well last most patient’s lifetimes.
The Australian Joint Replacement Registry and many literature publications show clear data confirming that more experienced surgeons usually have better patient outcomes.
The most important factor in determining long-term success of a hip replacement is to choose a skilled surgeon and be guided by his/her recommendations.
Every patient would like to recover as quickly as possible with as little pain as possible. Surgical and Anaesthetic techniques have improved significantly and these improved techniques have allowed an easier and faster recovery.
The Minimally Invasive Direct Anterior Approach (often termed DAA or AMIS) is an approach that may lend itself to a quicker short-term recovery due to the fact that the surgical approach uses intermuscular planes allowing exposure of the hip joint without detaching muscle off bone. This usually allows a patient the ability to recover quicker and return to function quicker compared to other approaches.
There are many published articles that have confirmed that the anterior approach usually leads to a quicker short-term recovery HOWEVER all published articles also confirm that after 6-12 months patients having had a successful hip replacement, function equally well no matter what approach is used.
The Australian Joint Registry has shown that the revision rate between anterior and other approaches is the same percentage although the reasons for revision differ.
The most commonly used worldwide approach to hip surgery is the Posterior Approach (ie from the back) and published results show there is no significant difference between a well done posterior approach and well done anterior approach at 12 months after surgery. The posterior approach requires splitting the gluteus maximus (buttock) muscle and detachment of the short external rotator muscles and then reattachment of these muscles/capsule and hence the slightly slower recovery compared to the anterior approach.
There are some short-term hip movement restrictions in the posterior approach (internal rotation of the hip beyond 90 degrees of flexion) for 6 weeks to prevent hip dislocation whilst the capsule/muscle repair recovers. The anterior approach is inherently a very stable approach not requiring muscle repair and movement restriction. Patients usually can return to driving at an earlier stage (1-2 weeks) if they have had an anterior approach. There are also no hip movement precautions during recovery.
Important Information
As an experienced hip surgeon (over 25 years performing more than 13000 hip and knee replacements) and I am very comfortable performing either the anterior or posterior approach for the arthritic hip. My general preference is to perform the minimally invasive anterior approach unless there are contra-indications.
HOWEVER
Not all patients may be suitable for the anterior approach due to many factors including:
- Morbid Obesity where the stomach overhangs the front of the hip.
- Abnormal anatomy (such as Hip Dysplasia, Perthes, previous fractures, abnormal bone structure etc.)
- Severe osteoporosis.
- Significant muscular build resulting in very tight and limited joint visualisation.
- Significant leg length discrepancy.
- Deficient bone requiring bone grafting or augmentation of the socket.
- Specialised hip implants needing to replace the hip joint.
- Most revision hip surgery unless a simple head/liner exchange or loose stem/cup.
The Responsible Approach:
Every patient I see has an individual assessment taking into account their hip pathology, degree of arthritis, day to day function, general health and body habitus. I will then advise what I believe to be the best surgical approach to achieve the best clinical outcome with the least chance of a complication.
Whilst I would prefer from a general recovery perspective to perform an anterior approach it is MORE IMPORTANT to ensure a safe recovery with appropriate attention to the underlying problems at hand. If I feel that the anterior approach is not suitable, I will perform a posterior approach AND will reassure the patient that whilst they may have a slightly slower recovery compared to the anterior approach, their LONG-TERM function will be identical.
Rehabilitation following Hip Replacement:
Many patients DO NOT require formal in-patient rehabilitation and can be discharged home with outpatient physiotherapy and a home-based exercise program. Studies have conclusively shown that there is NO difference in outcomes between inpatient and outpatient rehab.
There is a false perception that by not going to in-patient rehab your result will be inferior. This is simply NOT TRUE and many published studies have proven that home discharge is as good. It is not that I am against in-patient rehab, rather the point I make is that especially for hip replacements (as apposed to knee replacements), in-patient rehab for most people offers no advantage to out-patient rehab. There are off-course exceptions.
I encourage patients to go home following surgery however there are patients who benefit from in-patient rehab when home circumstances are not ideal or where extra medical attention is required.
How long will my hip replacement last?
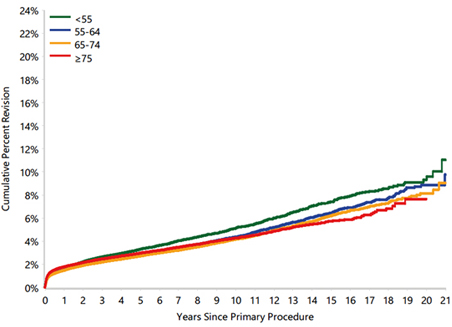
This is naturally a very common question. The main determinates that effect outcome are Age and Implant Type. There is no clearcut answer however using tried and tested implants with modern day bearings, the replacement is likely to last 25 years or more.
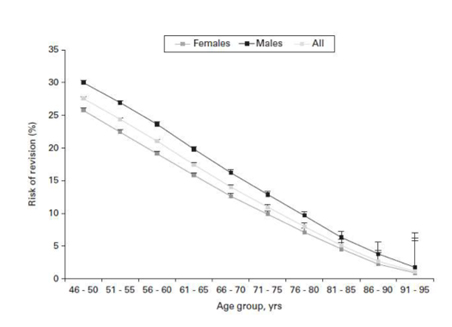
Below are 2 graphs. One is the Australian Joint Registry Revision rate based on age at time of replacement and the other is from the New Zealand Registry that takes into account the life expectancy of a patient and the revision risk based on their age and life expectancy.
-
 Australian Joint Registry 2022 data
Australian Joint Registry 2022 data -
New Zealand Life Expectancy Study
The Final Word……..
The key to a successful hip replacement with the best chance of a good functional outcome and the least chance of complications is to choose an experienced skilled hip surgeon. Whilst the Anterior Approach may afford a quicker short-term recovery, not all patients are suitable for this approach, yet be reassured that at 6-12 months the posterior approach performs equally as well.
Bearing Surfaces:
The main bearing surfaces (moving parts) are the following:
- Ceramic on highly cross-linked polyethelene
- Metal on highly cross-linked polyethelene
- Ceramic on Ceramic
- Duel-Mobility
- Metal on Metal Resurfacing
Hip replacement implants have been around for over 50 years and over the past 50 years scientists and the orthopaedic community have developed bearing surfaces that are now much longer lasting and likely not to require revision for wear-related problems in the majority of patients. In other words, most patients needing hip replacement surgery over the age of 60 are unlikely to require revision hip surgery for a bearing failure.
The latest Australian National Joint Registry (2022) results show that after 20 years the following revision rates apply to bearing surfaces:
- Ceramic on highly cross-linked polyethelene: 6.8%
- Metal on highly cross-linked polyethelene: 7.7%
- Ceramic on Ceramic: 9.3%
D: Metal on Metal Resurfacing in Males: 7.7% - Duel-Mobility at 10 years is 5%. There is only 10 year data available. At 10 yrs Ceramic on highly cross-linked polyethelene revision rate was 4%
It appears that the most durable and “safe” bearing for the majority of patients is ceramic on highly cross linked polyethelene. Duel-mobility bearings have a higher revision rate in young patients and this bearing is best used when there is a high risk of instability in a particular patient.
Whilst larger femoral heads and duel-mobility bearings have a theoretical improved range of motion, the reality is that a well-positioned hip replacement will have good flexibility and stability with any head size 32mm and above.
Treatment Journey:
First Consultation: Please complete the patient form prior to the consultation.
Dr Solomon will take a history and examine the hip and review any investigations or order additional radiological investigations.
All hip replacements will have an OPS X-Ray evaluation to best determine the appropriate sizing and component alignment. This test is done at i-med radiology next to Dr Solomon’s office and is bulk billed.
You can read about the OPS system using this link: Optimized Positioning System™
Preparing for surgery:
- Please contact the pre-admission clinic for routine blood tests and a general health check. You will be provided with contact details.
- Purchase an Antiseptic liquid Body Wash (Microshield 2 Chlorhexidine Skin Cleanser ) and use as a body wash in the shower for 2 days prior and the morning of surgery.
- Cease all blood thinning medication warfarin, aspirin, plavix, fish oil, glucasamine and herbal medication as advised. If you are on long term blood thinning medication I will liase with your cardiologist / GP about the timing as to when to cease these medications and if you need alternative cover.
- Diabetic Medication: You need to cease the following medication 3 days before surgery: Jardiance, Jardiamet, Forxiga, Quern, Glyxambi, Xigduo XR, Stelatro, Segiuromet, Steglujan, Invokana.
- If you are due to have dental work, routine colonoscopy or prostate procedures, please have this done at least 4 weeks prior to your hip surgery.
- Blood Iron and Vit D Level: It has been shown that having normal iron levels and vitamin D levels will result in reduced complications. Your blood tests prior to surgery will test for these levels and if they are low, you will need to take a supplement.
- Skin/Nasal swab. As a routine I test for skin organisms. We all carry organisms on our skin. The bodywash pre op is to reduce the skin organism count. Occasionally the pre-op test will pick up a methicillin sensitive staph or a methicillin resistant staph. The DOES NOT mean you are infected but rather these bugs are on the skin. It may mean the hospital will take extra precautions with nursing care. You will be prescribed an ointment for 48 hrs to use in your nose (mupericin) to decolinise the nares.
- Smoking should be stopped or reduced significantly prior to surgery as smoking has been shown to be associated with increased complications.
Procedure:
- Anterior Total Hip Replacement
- Posterior Total Hip replacement
- Birmingham, Adept and Ceramic Hip Resurfacing
- Peri-Acetabular Osteotomy
Post Hospital Care:
You will either be discharged home or into an in-patient rehab facility. You will be given pain medication, blood thinning medication to prevent thrombosis and a crutch or walking stick to be used for 4 weeks. As mentioned before, in-patient rehab and home-based outpatient rehab have the same outcomes in hip replacement surgery. The majority of patients prefer outpatient rehab and head home. Hip replacements do not need a lot of physio/ rehab exercises so don’t overdo the exercises. Time will heal.
Rehabilitation:
In-patient rehab and home-based outpatient rehab have the same outcomes in hip replacement surgery. The majority of patients prefer outpatient rehab and head home. You will be given pain medication, blood thinning medication to prevent thrombosis and a crutch or walking stick to be used for 4 weeks. Hip replacements do not need a lot of physio/ rehab exercises so don’t overdo the exercises. Time will heal.
This link shows useful hip exercises: Total Hip Replacement Exercise Guide
